Dr. James Cowan has seen how health insurance works from multiple angles and both sides of the pond, consulting for the National Health Service, the United Kingdom’s public health-care system, to serving as an expert for the health-care insurer Aetna here in the United States. Now acting as an advisor for the Rhode Island Health Care Access and Affordability Partnership (RIHAAP), his mix of perspectives informs one of his central, and perhaps most surprising, arguments for single-payer health care: universal coverage is actually much better for our country’s businesses and economy.

Dr. James Cowan
“The only way to make health insurance accessible to everybody in the country—assuming that’s what you want to do—is to put everybody in a group of some kind,” Cowan said. “And the most efficient way to do that is to put everybody in a single group. And the best example of that is Medicare, which currently insures around 65 million Americans, with customer satisfaction higher than any private insurance company.”
Cowan put it to me like this: suppose you want to insure your house. You know the worth of your house, and experts happen to know the rate at which houses burn down every year, so your premium is simply the first number divided by the second, to account for the percentage of risk among a group of homeowners with the same insurance. This keeps premiums relatively low—fewer houses burn down every year versus the number of people who have house insurance—and because it is indexed to the price of your house, those with more expensive homes who are able to pay more for a premium will naturally do so.
What is especially important is that homeowners are put into a group that calculates the rate of homes going up in flames, and the larger the group, the more the cost of burned-down houses will be spread across each plan, and the lower the premium for each.
Everything changes when you want to insure your body. We might still know the the rate of risk for certain conditions or illnesses among a certain group: Cowan gave an example estimate that 1 in 400 people get appendicitis every year (the actual national rate is much lower), and a treatment for appendicitis might cost $4,000. You can then say that the premium for appendicitis is roughly $10 for that group, and add it to the premium for all sorts of other potential ailments. And again, the larger the group, the better, because then insurers can be more sure that they can cover the costs for those who do wind up with the disease.
This, Cowan said, is precisely the reason why health care in the US does not work for individuals—especially the unemployed or those who do not receive insurance through their employment—or owners of small businesses, which make up the vast majority of employers in the US according to the Small Business Association. If a group of insured people is too small, or if a person isn’t in a group at all, insurance companies cannot easily calculate the cost of insuring an individual because they don’t know what illnesses this individual might get in the future. This is “made worse by the fact that what insurance companies do then is try to guess who’s going to get sick, and then not insure them or charge them an exorbitant premium. And then on the other side, people who think they’re not going to get sick don’t get insurance, which drives up the cost for everybody else,” as Cowan argued.
Health care also makes up a “significant portion” of small businesses’ labor costs, with the average family plan now at $24,000 a year—expenses that would be rolled back under universal coverage.
The problem lies not only with the nitty-gritty of how premiums are calculated, but with the inefficiency of private insurance companies themselves. Cowan estimated that for private enterprises, overhead costs make up around 15-20 percent of the premium, as compared to 2% under Medicare. This is due to the mountains of paperwork involved—considerations like the dates of coverage, and the providers in each company’s network—that isn’t factored into a continuous Medicare plan where most health-care providers are in-network. It’s also because health insurance companies require a far larger marketing budget and sales team. All in all, Cowan told me that as the US spends $3.3 trillion on health care every year, 15% in overhead costs means around $700 billion, “about equal to the entire spending on the Department of Defense this year.”
After adding that it is “widely accepted” that 33 cents out of every dollar spent on health care does not improve someone’s health, it was at this point in his explanation that Cowan, to use his turn of phrase, “put on his libertarian hat.” If employers don’t hire labor to do nothing a third of the time, or buy from suppliers which wastes a third of their supply chain, why would you settle for 33% waste in health care?
I ruffled a little at this, and asked if this meant that a third of those employed in health care—the largest source of jobs in the US according to the Atlantic—could lose jobs deemed unnecessary if administrative roles were rolled back under single-payer. He conceded that they might, and “politically, this is obviously a problem—it would be cruel.” But he added two stipulations: the first is that you could implement a more universal system gradually, allowing for a smoother adjustment. But the second stipulation, and what many don’t realize, is that it would easy for some workers to transition to working under Medicare for All because both Medicare and Medicaid already contract out its administrative functions to private insurance companies, who have spent the overhead to develop technology to handle claims.
As for the argument that costs would be driven down with increased competition—as in proponents of letting out-of-state insurance companies compete with those in Rhode Island—Cowan argued that this was largely a myth. This is because insurance companies “are price takers, not price makers,” meaning that it is largely health-care providers—hospitals and drug companies, for instance—which set the price of services. Cowan reported that typically, Medicare makes up 50 percent of providers’ revenue stream, Medicaid taking up another 20 percent, and state Blue Cross Blue Shield plans another 15 percent. This leaves other private insurance companies with a far reduced negotiating power—and increased competition among them would only exacerbate the problem.
“If you’re going to drive that down, you need to get a better negotiating position with providers, which you’re not going to do by bringing more insurers in,” Cowan said. “ You want to reduce the number of insurers, and ideally, if you only had one insurer, if you just had Medicare for All, then you’d have a very powerful position with negotiating over prices with providers.”
Cowan went on to assert that this is why the American Hospital Association and drug companies “are going to oppose Medicare for All like crazy,” as it would drive their prices down.
This is, perhaps, where an argument by-the-numbers might end, and a political movement—one that pits humane values against those vested in growing profits—might begin instead.
CORRECTION: A previous version of this article stated that insurance companies cannot easily calculate the risk of any illnesses for individuals. In fact, it is that they cannot calculate what future illnesses an individual might get.



 Conservation Law Foundation (CLF) filed a lawsuit today against ExxonMobil for its endangerment of communities along the Mystic River – the first lawsuit of its kind in the nation since revelations last year about the corporation’s decades-long campaign to discredit climate science. Today’s filing comes several months after CLF submitted a formal letter of intent to sue ExxonMobil,
Conservation Law Foundation (CLF) filed a lawsuit today against ExxonMobil for its endangerment of communities along the Mystic River – the first lawsuit of its kind in the nation since revelations last year about the corporation’s decades-long campaign to discredit climate science. Today’s filing comes several months after CLF submitted a formal letter of intent to sue ExxonMobil, 

 Raimondo has consistently touted her support for renewables like wind and solar, only occasionally voicing her support for fracking. Raimondo never holds a press release in front of a fracked gas pipeline or compressor station. She holds them at wind turbines and solar farms, giving the appearance of a strong leader on the environment.
Raimondo has consistently touted her support for renewables like wind and solar, only occasionally voicing her support for fracking. Raimondo never holds a press release in front of a fracked gas pipeline or compressor station. She holds them at wind turbines and solar farms, giving the appearance of a strong leader on the environment. Catholics for Choice has released a
Catholics for Choice has released a  The candidacy of Donald J. Trump for President of the United States finds daily a new road to Hell, and threatens to drag the nation, and the world, down with it.
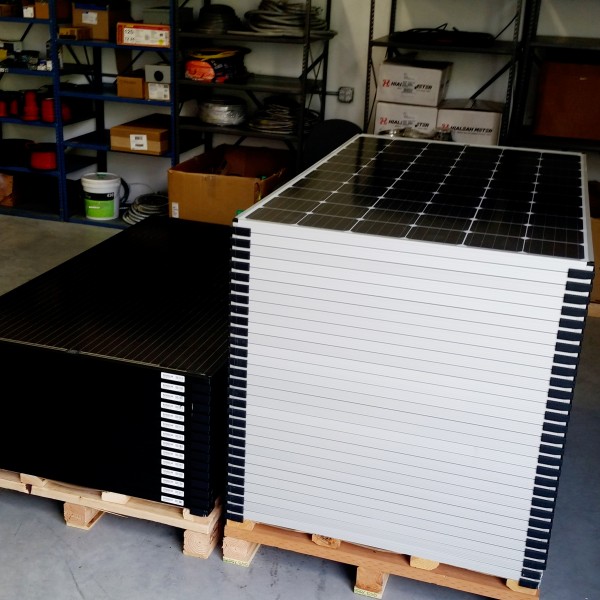
The candidacy of Donald J. Trump for President of the United States finds daily a new road to Hell, and threatens to drag the nation, and the world, down with it.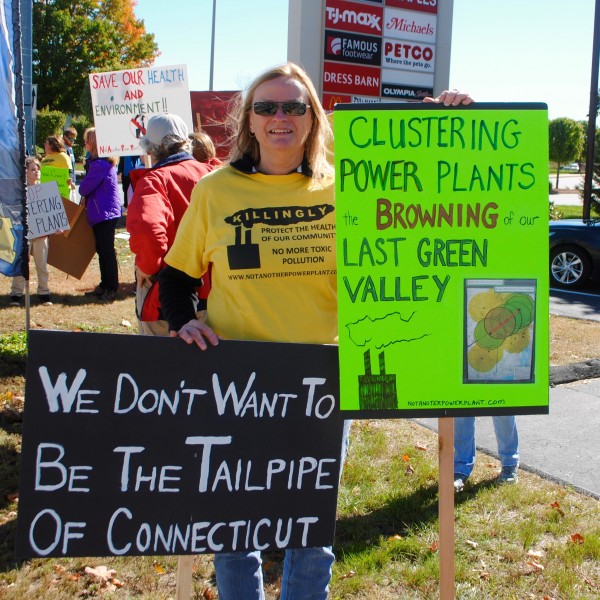 As large as Invenergy‘s $700 million fracked gas and diesel oil burning power plant would be if it were to be actually built in the pristine wilderness of Burrillville, the project is but a small part of a colossal, three-state fracked gas infrastructure project that has been in development for years in the northwest corner of the Rhode Island and beyond. Eight power plants currently litter a 31 mile expanse of pipeline, from Killingly, Connecticut, through Rhode Island, to Medway, Massachusetts. If built, Burrillville would be power plant number nine and Killingly is the proposed site of power plant number ten.
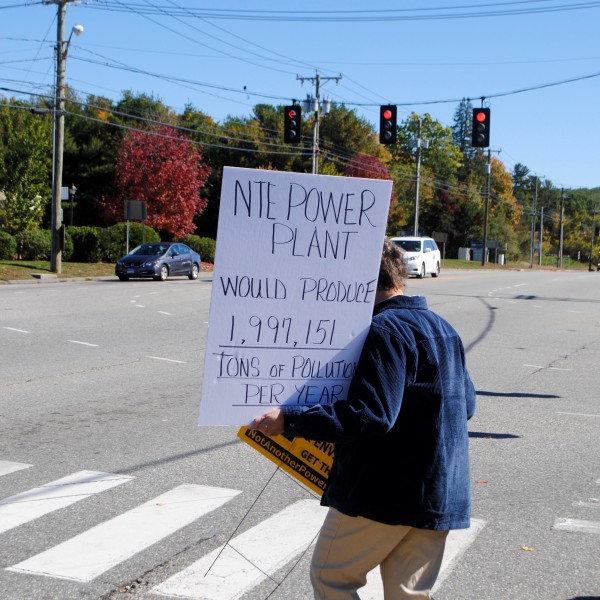
As large as Invenergy‘s $700 million fracked gas and diesel oil burning power plant would be if it were to be actually built in the pristine wilderness of Burrillville, the project is but a small part of a colossal, three-state fracked gas infrastructure project that has been in development for years in the northwest corner of the Rhode Island and beyond. Eight power plants currently litter a 31 mile expanse of pipeline, from Killingly, Connecticut, through Rhode Island, to Medway, Massachusetts. If built, Burrillville would be power plant number nine and Killingly is the proposed site of power plant number ten. The Killingly power plant is to be built in a residential neighborhood within a mile of 460 Killingly housing units. At least five schools and day cares, over 5,000 students, are within three miles of the proposed plant. Wyndham County, where Killingly is located, has asthma rates 18 percent higher than the rest of Connecticut.
The Killingly power plant is to be built in a residential neighborhood within a mile of 460 Killingly housing units. At least five schools and day cares, over 5,000 students, are within three miles of the proposed plant. Wyndham County, where Killingly is located, has asthma rates 18 percent higher than the rest of Connecticut. The Town of Killingly is categorized as a distressed community. Like other areas where these types of facilities are targeted, there are environmental justice issues to be considered. Very often the facilities are like these are aimed at low income communities that lack the financial means to either fight the power plant or resist the financial carrots dangled by the company building the plant.
The Town of Killingly is categorized as a distressed community. Like other areas where these types of facilities are targeted, there are environmental justice issues to be considered. Very often the facilities are like these are aimed at low income communities that lack the financial means to either fight the power plant or resist the financial carrots dangled by the company building the plant.
























 In order to fund their ideas, the CIW asked corporation to pay an extra one cent per pound of produce purchased. This money would allow the workers to push for higher wages and establish a code of conduct that contained zero tolerance for the worst abuses. This allowed workers to demand respect, and in fact they mandated that the worker’s voices be heard during the implementation of these changes.
In order to fund their ideas, the CIW asked corporation to pay an extra one cent per pound of produce purchased. This money would allow the workers to push for higher wages and establish a code of conduct that contained zero tolerance for the worst abuses. This allowed workers to demand respect, and in fact they mandated that the worker’s voices be heard during the implementation of these changes. Today 14 corporations are signed on, but CIW is looking to expand this program of Worker Driven Social Responsibility. They have expanded beyond Florida and into other states such as Georgia and North and South Carolina. They have expanded beyond tomatoes and into other crops such as strawberries and bell peppers. They want more corporations to sign on.
Today 14 corporations are signed on, but CIW is looking to expand this program of Worker Driven Social Responsibility. They have expanded beyond Florida and into other states such as Georgia and North and South Carolina. They have expanded beyond tomatoes and into other crops such as strawberries and bell peppers. They want more corporations to sign on.

 Nearly three dozen people marched and chanted outside Wendy’s on Charles St in Providence Friday afternoon to call attention to the boycott of the food chain called by the Coalition of Immokalee Workers (CIW), a group that has fought for farmworker’s rights and fair treatment for two decades. Wendy’s remains the largest fast food chain that refuses to ethically source their produce from CIW supported growers. Rather than supporting the
Nearly three dozen people marched and chanted outside Wendy’s on Charles St in Providence Friday afternoon to call attention to the boycott of the food chain called by the Coalition of Immokalee Workers (CIW), a group that has fought for farmworker’s rights and fair treatment for two decades. Wendy’s remains the largest fast food chain that refuses to ethically source their produce from CIW supported growers. Rather than supporting the 










 The FANG Collective staged a demonstration outside TD Bank Wednesday to protest the company’s support of the Dakota Access Pipeline (DAPL), which is even now being blocked by First Nation protesters from many different tribes. TD Bank is one of many lending institutions financing the pipeline.
The FANG Collective staged a demonstration outside TD Bank Wednesday to protest the company’s support of the Dakota Access Pipeline (DAPL), which is even now being blocked by First Nation protesters from many different tribes. TD Bank is one of many lending institutions financing the pipeline. This protest follows an
This protest follows an  Protesters handed out flyers and held signs. One woman, Amy, after hearing from protester Sally Mendzela about the bank’s involvement with DAPL, told me that though she had come to open an account with the bank, she was not. Mendzela said that the woman was the second person to be dissuaded from doing business with TD Bank since she arrived.
Protesters handed out flyers and held signs. One woman, Amy, after hearing from protester Sally Mendzela about the bank’s involvement with DAPL, told me that though she had come to open an account with the bank, she was not. Mendzela said that the woman was the second person to be dissuaded from doing business with TD Bank since she arrived.











